This is a post to respond to a recent blog written by Sheena Byrom. The blog makes four points which I felt compelled to respond to. I address each of these points below (original message in black text and my response in blue) .
1.The Royal College of Midwives discontinued the Campaign for Normal Birth (CNB) THREE YEARS AGO. I was actually part of that decision, and it was due to the fact that the College felt it was important to encompass antenatal and postnatal care within the initiative, and public health. So ‘Better Births’ was born. It had nothing to do with the Morecambe Bay Report, which was published after the decision had been made. But even though the ‘Campaign’ ceased, the support for normal birth has not. The RCM have a normal birth resources page. Some of the resources developed for the CNB have been removed following a request, and will hopefully be replaced with more up to date material. Since writing this post, Cathy Warwick CBE, CEO of the RCM, has written to confirm the College’s continued position to support midwives to promote and facilitate normal physiological birth.
Response:
Whilst the RCM introduced its Better Births campaign 3 years ago, the RCM’s normal birth campaign website was kept live until May this year. There was no announcement by the RCM about removing the website in May. Key documents however, including the RCM’s ‘top tips for normal birth’ were transferred to the new Better Births website. Only in the last few weeks was this document, along with others removed.
For me, the most interesting and ‘news worthy’ parts of the reporting in the media were the quotes from the RCM CEO Cathy Warwick. These included the statement that the normal birth campaign “had the potential to be misleading”. Cathy also called the ‘top tips for normal birth’ document “just not professional enough” adding “..they have gone; they won’t be reintroduced in any way and we’ll have much more professional, evidence based guidelines for midwives.”
Cathy also acknowledged that the language of ‘normal birth’ could make some women feel like failures saying: “It does seem that this word ‘normal’ is particularly contentious . . . it is simpler to use a non-value-laden word. Because of the inferences that are drawn there will be instances where you’re explaining your position better by using terms like ‘physiological birth”.
As far as I have seen, most people have welcomed the news as reported and the comments from Cathy as being sensible and helpful.
When I tweeted the headline in the Times newspaper on Saturday 11th, comments from most were welcoming and positive. At Morecambe Bay for example, the response was ‘great news’ and confirmation that through listening to mothers, they had made changes in their language and approach some time ago.

2. THERE IS NO EVIDENCE that the RCM’s Campaign for Normal Birth had any direct influence on the tragedies that occurred at Morecambe Bay, or any other service. The adverse events at Morecambe Bay were attributed to five elements of dysfunctionality, one of which was the ‘over-pursuit of normal birth’. The report does not apportion blame to any one of the five individual elements, but to the whole five. In any case – why is the one element linked to resources supplied by the RCM?
Response:
I take strong issue with this.
An independent investigation was commissioned into the maternity services at Morecambe Bay which reported in March 2015. This found that 11 babies and one mother died avoidably at FGH. The report identified (amongst a number of other serious issues) that “care in the unit became strongly influenced by a small number of dominant individuals whose over-zealous pursuit of the natural childbirth approach led at times to inappropriate and unsafe care”. The report also quoted one midwife as saying “…there were a couple of senior people who believed that in all sincerity they were processing the agenda as dictated at the time… to uphold normality.”
It isn’t ever going to be possible to make a direct link to a campaign and individual cases of harm, but I have always believed that the RCM campaign has been an influencing factor in some of the clinical problems that developed at FGH. I have written about this long before the Kirkup report was published.
Today however, the Chair of the Morecambe Bay Investigation himself has intervened and published a letter in the HSJ which specifically addresses this point:
“One of those elements that crops up is the misunderstanding or misapplication of national guidance on promoting normal birth. I can’t say for sure that the RCM’s previous advice contributed to this, but some of the messages, particularly about waiting and seeing and trusting intuition, had clear echoes in what we heard at Morecambe Bay. The change in position [from the RCM] is welcome, and should not be undermined by optimistic and unlikely denial that such problems exist. We should continue to be explicit about the need for effective team work, explanation of risk, and looking and learning when something goes wrong.”
I would argue that as Bill Kirkup himself has highlighted the very messages in the RCM campaign “had clear echoes in what we heard”, it would be extremely unlikely that the RCM campaign was not an influencing factor.
The blog also states there is no evidence of this issue impacting on care in “any other service”. Actually there is evidence that that parents who have lost children and professionals dealing with claims relating to brain damaged babies feel that this exact issue is a real and significant contributory factor.
For example, please read this blog from Leigh day solicitors or this report and the comments from families whose babies died following failure in care at SaTH.
In the last week, I’ve been amazed at how many families have shared their stories. If you doubt me, read the responses to this tweet – Yes, of course this is anecdotal – but is it right to just dismiss the experience of all these women and families?
A final relevant link is here. This was shared with me today by a mother who lost her baby son in the Netherlands. Please read it. It highlight very similar issues in a country whose equivalent of the RCM (the KNOV) have implemented a very similar normal birth campaign.
3. I believe in choice, autonomy, and safety. Out of our 9 grandchildren, none have been born ‘normally’. They needed expert medical intervention, medical support, and I am eternally grateful for the attention they received. I also understand the evidence that physiological normal birth is the optimal way to give birth for most women, and that most women want it.
To make informed choices women need to have accurate information, including honest information about risk not misrepresentations as described here. Information must also be unbiased and not leading, as discussed here. Top down messages aimed at only one profession vital to ensuring safe maternity care, such as ‘wait and see’ and ‘trust your intuition’, surely don’t help ensure women and babies receive timely lifesaving interventions when needed. I have never argued against the very valid and important objective of aiming to reduce unnecessary interventions. I have argued that this objective must be implemented in a way that doesn’t increase the risk of catastrophic outcomes for some.
I wrote this blog in 2014 which describes a number of reports into the causes of adverse neonatal outcomes (death and serious injury). The themes are clear.
No one disputes that ‘physiological’ birth will be the optimal way to give birth for most women. The issue here is that it is never possible to know for certain if a safe, physiological birth is possible until after the birth. Before then, there is only a spectrum of risk. The World Health Organisation (WHO) estimates that in 12-15% pregnancies, women suffer life-threatening obstetric complications. My argument is that the RCM’s normal birth campaign and documents like the ‘top tips for normal birth’, should be replaced with more balanced messages involving all professionals needed to deliver safe maternity care.
4. I hear and fully respect that some women feel that the word ‘normal’ in relation to birth is divisive, and upsetting, leaving them feeling like they ‘failed’. I can understand this, that women may feel disappointed if they wanted a particular birth experience, worked towards that goal, then it didn’t happen. But that’s it. I would like to suggest that it is the end result is the disappointment, more than the word. Would women feel less disappointed if birth was called physiological? I liken this debate to infant feeding. If a woman has problems and ceases to breastfeed her baby, she feels disappointed – no matter what the term is. Normal birth is a normal physiological bodily process – as is normal respiration, and digestion. The terms physiological, natural and any other are fine too, but let’s not blame a word for disappointment. We need to listen to the experiences of women when they are unhappy with their birth experience for whatever reason, then aim to change services so that optimal childbirth is the goal, for a healthy mother and baby. I will not stop using the term ‘normal birth’ and I will support midwives to facilitate women’s choices safely.
Response:
I would respectful disagree that the reason some women feel like they have ‘failed’ is simply because they are disappointed by the ‘end result’. As a man, I’m not in a position to know how women feel, but I have read dozens of comments from professionals and women in recent days and I have listened to what they say. Themes include what woman are told in anti-natal classes through to actually been told they have failed because they needed pain relief or intervention.


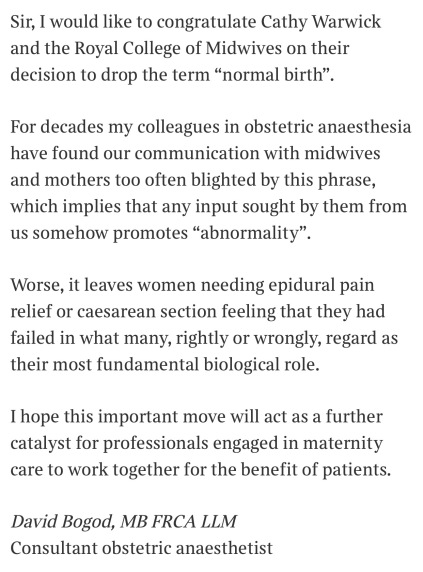
A respected consultant obstetric anaesthetist, Doctor Bogod wrote the following letter in the Times last week:

This letter was dismissed as “rubbish” on twitter by one senior NHSE employee, but is this really an entirely made up issue? In a compassionate, kind and caring NHS, shouldn’t the experiences of woman and other healthcare professionals be listened to? If women and healthcare professionals are asking for different language and saying that they feel ideology is getting in the way of unbiased information, being truly empowered to make their own choices, and the safety of their care, shouldn’t those working in maternity services be open to listening?



James Titcombe – 21/8/2017