In October 2008, our world was different. Our daughter Emily was just three and a half years old and at the time I was working as project manager at a large nuclear site in Cumbria. At 7.38am on 27th October 2008, our second child Joshua was born at Furness General Hospital (FGH), part of the Morecambe Bay NHS Trust. I remember staring at him in his cot, thinking how perfect he was and how lucky I was – how lucky we all were. But just 24 hours later – that world ended.
An early morning phone call broke the news. I remember the words as if it was yesterday…
“Joshua is having problems breathing and your wife is very upset – can you come to the hospital”
I remember phoning my mum and hearing her voice break (mums have an instinct), getting to the hospital and seeing Joshua in the Special Care Baby Unit – initially breathing by himself but quickly put on a ventilator as I’m ushered out the room. Confusion, uncertainly, desperation, fear, hope and despair followed.
Joshua was transferred by ambulance to a specialist unit in Manchester and my wife and I followed him by car. At this point we were uncertain as to what was wrong. We were told there might be a problem with his heart or his oesophagus, but even then, these explanations did not seem to fit.
My wife had been feeling unwell in the days before Joshua was born and shortly after his birth, she collapsed with a high temperature and was given intravenous fluids and antibiotics. She recovered quickly, but we both raised concerns with staff about Joshua – if my wife needed antibiotics, wasn’t Joshua also at risk of infection? Despite raising these concerns with staff, we were repeatedly reassured that ‘Joshua was fine’.
Surely his collapse 24 hours later could not be due to infection? Not after we had specifically raised concerns with staff about this and been reassured repeatedly that Joshua was ok.
The following day the team in Manchester confirmed our fears; Joshua had collapsed due to an overwhelming pneumococcal infection – the same strain that had now been identified as having caused my wife to collapse shortly after the birth. Questions about how this could have happened raced around my mind. Could I have done more to raise concerns and insist Joshua was seen by a paediatrician sooner? These feelings of regret and guilt have never left me.
But these questions had to be put on hold for now. Joshua was still fighting for his life and all that mattered was getting him the right care and treatment so we could bring him home.
At Manchester we were told that Joshua’s best option was to be flown to a specialist unit in Newcastle to be put on a heart and lung machine for babies. The treatment had risks but the unanimous view of his clinical team and our family, was that this treatment would give Joshua the best chance of recovery.
Joshua was flown by helicopter to Newcastle and for a final time, my wife and I followed him by car. When we arrived in Newcastle, Joshua had already been hooked up to the medical machinery that we hoped would save his life. We were greeted by a kind consultant who told us that Joshua’s prognosis was good and showed us a wall of cards, letters and photos from the families of other children who had been cared for of the unit and had recovered and were now doing well at home with their families.
We had 7 hopeful days in Newcastle, Joshua sedated but able to open his eyes and squeeze a finger.
We hoped that we would get to take our baby boy home too, but that was not to be. Those hopes were dashed when he died at just 9 days old as a consequence of internal bleeding caused by the damage the pneumococcal infection did to his lungs.
Although over a decade has passed since these moments, I remember them as vividly as if they had happened just yesterday. Seeing Joshua for the first time after his death with all the tubes and medical equipment removed – he looked like a perfect baby boy. How could he have died for want of a simple dose of antibiotics at the right time?
The loss of any child in whatever circumstances is a life changing tragedy – but coming to terms with Joshua’s death was made incalculably worse by the way the trust and healthcare system responded.
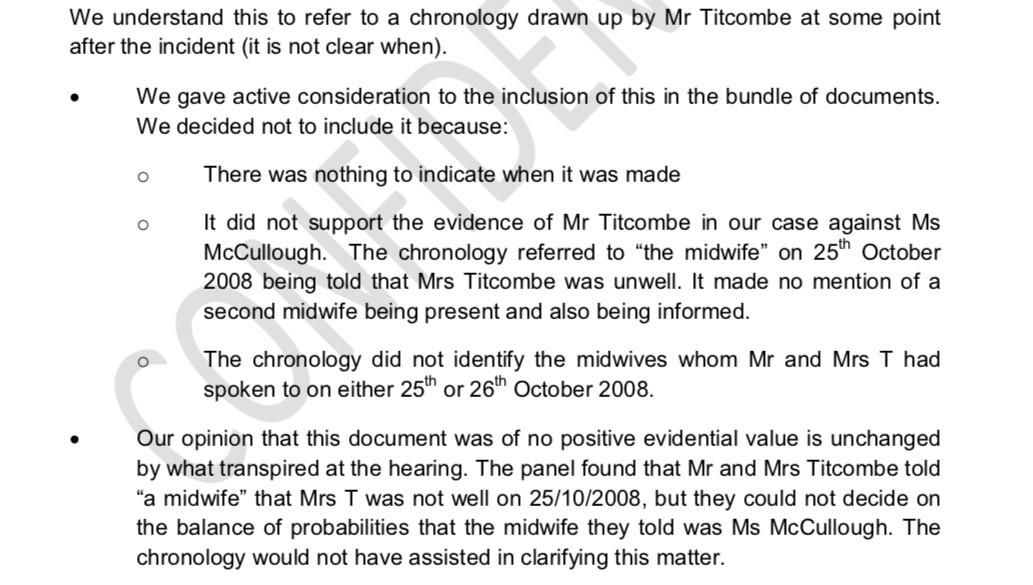
Crucial medical records of Joshua’s observations went ‘missing’, staff accounts of what happened at Furness GeneralHospital conflicted with the events as my wife and I remembered. The initial report from the hospital concluded that Joshua’s observations in the 24 hours after his birth before he collapsed were all within ‘normal’ limits and that therefore no one was to blame for what happened.
As Joshua’s father, I could not accept these false narratives. I had failed to keep Joshua safe during his short life, but I wasn’t prepared to allow the truth about his death to be swept under the carpet. I soon discovered that the healthcare system, it seems at almost every level, was not open to looking for, let alone acknowledging the truth about what happened to Joshua and why.
The journey since has been long, hard and at times lonely, but eventually we did establish a truthful account of what happened to Joshua and in doing so uncovered a far wider scandal at the maternity unit where he was born. After meeting other families who had experience of tragic outcomes following poor care at same unit, I started a campaign group and worked to try and secure a national inquiry into the safety of the unit. The campaign was successful and the Morecambe Bay Investigation report, chaired by Dr Bill Kirkup was published in March 2015.
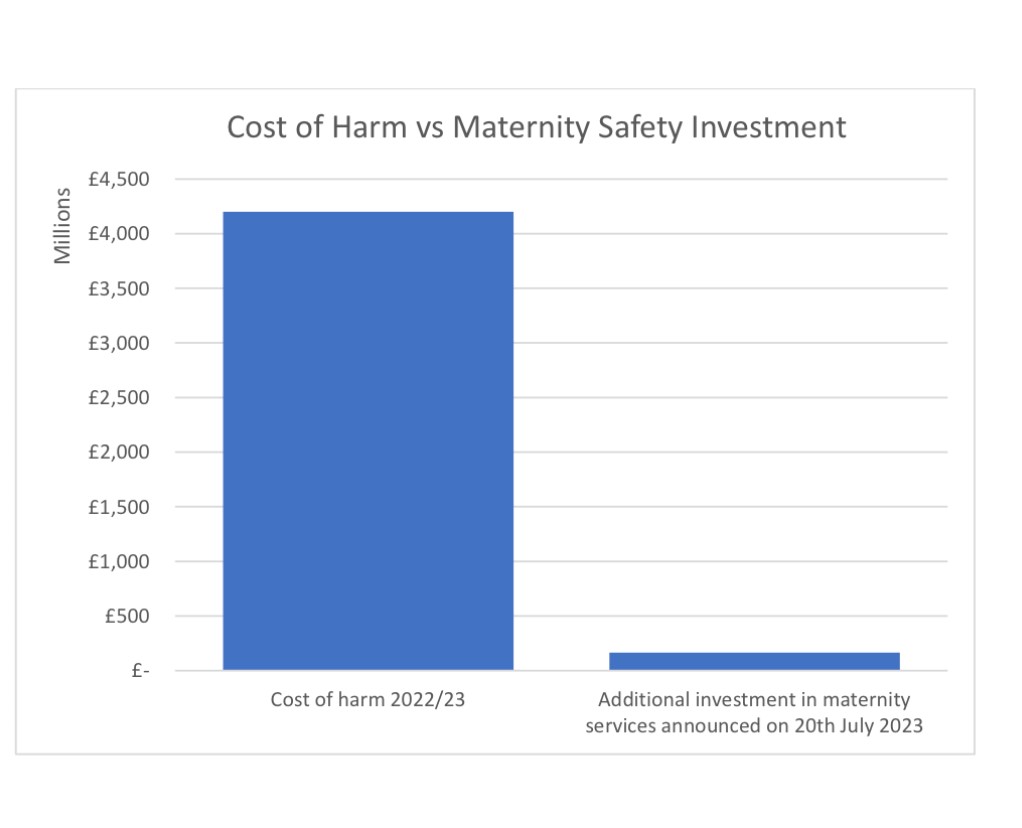
The report concluded that between 2004 and 2012, a ‘…lethal mix of failures’ had led to the avoidable death of 11 babies and 1 mother at Furness General Hospital – Joshua was just one of many preventable deaths. It described the maternity unit where Joshua was born as characterised by ‘…denial and cover up…’. The report made 26 recommendations for national change and triggered a programme of work in England with the aim of halving avoidable harm in maternity units across the country by 2025.
The maternity unit where Joshua was born no longer exists. It has been replaced by a brand-new facility, the South Lakes Birthing Centre which opened in 2017 – a state of the art unit designed with input from mums and families in the local area. Outside the new unit now stands a beautiful memorial to the 11 babies and 1 mother who Dr Kirkup found had died following serious failures in care. As well as remembering lost loved ones, the memorial is also a symbol of learning, forgiveness, and hope.
Amongst the national changes that have happened since the Morecambe Bay Investigation report was published, England now has a new Healthcare Safety Investigations Branch (HSIB). This new organisation has a remit to undertake national investigations into patient safety issues in the NHS, using a methodology that focuses on learning and not individual liability or blame. As well as this national work, HSIB now also undertakes independent investigations into the most serious cases of unexpected poor outcomes in maternity.
If what happened to Joshua happened today, an independent investigation focused solely on learning would take place without delay. It is hard to overstate the difference I believe this would have made – not just to our family, but to other mothers and babies as well as healthcare professionals at the trust.
One of the saddest revelations of the Morecambe Bay Investigation was that after Joshua’s death, 6 other babies died at the same unit due to a similar pattern of systemic problems in the way care was being delivered. As human beings, even when the consequences are life changing, I believe that most of us have the capacity to seek to understand and forgive individual, unintentional mistakes. But when faced with denial, cover-up and a failure to learn, forgiveness and resolution become almost impossible.
I no longer work in the nuclear industry and instead now spend my time working and campaigning for safer healthcare. Along this journey I have had the privilege to meet many other people who are working to improve patient safety, including other bereaved families who have trod a similar path. I now understand that our experience after Joshua’s death was not unique – the response we experienced and the battle we had to endure to establish what really happened and why – is sadly all too common, not just in our healthcare system, but in other healthcare systems around the world.
Although there has been some crucial progress in the years since the Morecambe Bay report was published, the NHS has still not succeeded in changing many of the key systemic issues that contributed to what happened at Furness General Hospital. In March 2020, the UK regulator of NHS hospitals, the Care Quality Commission (CQC) published a report which concluded that the issues identified in the Morecambe Bay Investigation ‘…staff not having the right skills or knowledge; poor working relationships between obstetricians, midwives and neonatologists; poor risk assessments; and failures to ensure that there is an investigation and learning from when things go wrong’, were ‘….still affecting the safety of maternity care today’.
Change can feel painfully slow, but I haven’t lost hope that we will one day reach a much better place in healthcare and be able to look back on stories like Joshua’s with a sense of incredulity that things could ever have been that way. But I do not believe that we will get there without a fundamental shift in the way healthcare systems manage patient safety risks and respond to harm.
What still needs to change?
In the aftermath of Joshua’s death, as well as struggling to deal with trauma and grief, I was also consumed with a burning sense of injustice and anger. The more I learned about the culture of the unit where Joshua was born, the more I realised that Joshua’s death was far more than an unavoidable accident. The Kirkup report concluded that the first opportunity that the trust had to identify serious systemic issues was following the avoidable death of another baby in 2004 – more than 4 years before Joshua died. But the investigation that was carried out by the trust was superficial, ‘…protective of the staff involved’ and failed to result in any meaningful action to learn from what happened and make the service safer for others.
We live in a world where human beings are prone to error and mistakes – but where that normal variation in human performance can lead to serious or catastrophic outcomes, for example the nuclear industry or in aviation, considerable effort is usually placed on designing and building systems and processes to prevent those mistakes leading to harm.
Joshua was born in a maternity unit characterised by dysfunction – staff lacked basic competencies and skills, processes and guidelines were out of date, midwifes and doctors perceived themselves to have different objectives and there was distrust and blame in place of teamwork and shared goals.
Overriding all of this was a leadership culture that was toxic to transparency, learning and improvement. The trust at the time was preoccupied with achieving ‘Foundation’ status, which would have given them greater control and financial freedom – but crucially this involved persuading various regulators that they met the appropriate standards of governance and quality. A seriously dysfunctional maternity unit with a history of avoidable harm was a problem that the senior leadership team sought to manage – they focused on doing everything possible to reassure the local community and regulatory system that their services were safe.
Unpicking all these behaviours is complex – the healthcare system at the time seemed to be influenced by perverse incentives – pursuing strategic objectives and meeting performance targets, seemly put above the safety of mothers and babies. But who was ultimately responsible for this culture and why was so little done to challenge it at the time?
In terms of the healthcare professionals who were looking after Joshua that fateful day, to what extent should they be blamed for what happened? Who was ultimately accountable for the system that allowed such a preventable death to happen? What processes should have been followed to respond to what happened? What duty of care was owed to Joshua’s family and the staff involved and what responsibility did the trust have to ensure every possible lesson from what happened was taken?
Over the years I’ve learned a great deal about how our healthcare system works. The simple truth is that existing systems, processes and regulatory incentives and levers often make it hard for healthcare professionals do the right thing. In the aftermath of harm, the relationship between the patient or bereaved family can almost instantly become adversarial. In Joshua’s case there was initially no inquest – we were told to raise our concerns about Joshua’s care via a formal complaint.
Rather than our family and the trust working together via a process to understand and learn, immediately the process became one of ‘allegations’ for the trust to respond to. This happened with oversight of the trust legal team whose remit is to carefully ensure that the responses that are provided protect the organisation from any admission of civil liability.
For individual healthcare professionals, the vast majority of tragic outcomes like Joshua’s death occur without any deliberate intent, but rather as a consequence of normal human performance/error and a combination of unsafe systems and processes. However, healthcare staff often have little faith that trust investigation processes will be candid about systemic problems and instead fear being singled out for blame or referral to a professional regulatory body.
Whilst none of these factors can justify acts of dishonestly or covering up, countering this fear is crucial if we want to create the kind of learning culture that has played such a decisive role in making other high risk sectors safer. Furthermore, the focus on inappropriate blame detracts from where clear and meaningful accountability should lie.
Although it took nearly 10 years, eventually I did manage to reach a point of reconciliation, healing, and some extent – forgiveness following what happened to Joshua.
After the Morecambe Bay Investigation report published, the trust agreed to carry out some further work around Joshua’s death. Although 8 years had passed, they carried out the kind of comprehensive investigation that should have happened if current best practice guidance was followed. The investigation highlighted serious failures that other external processes had already found but also issues with Joshua’s care and treatment that we were not previously aware of. But the crucial difference with this investigation was that the trust themselves had carried it out – for the first time since Joshua’s death, I felt confident that the trust themselves owned and understood Joshua’s story and therefore could be trusted to take it’s learning forward.
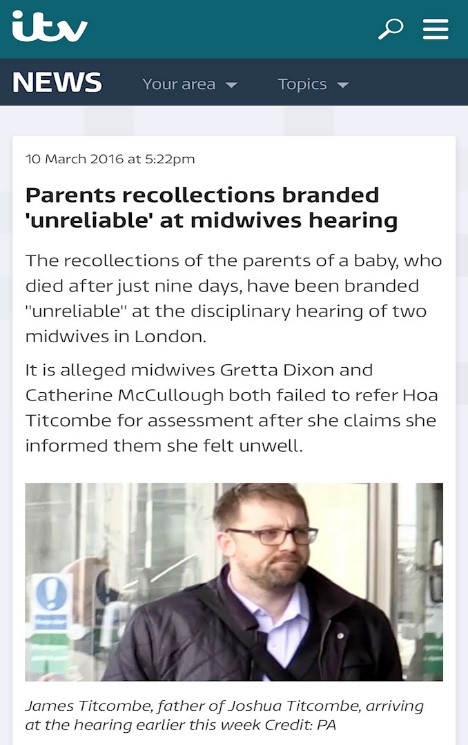
The final aspect of the work the trust carried out was by far the most difficult but also the most healing. A midwife who had a direct role in failures relating to Joshua’s care had been heavily criticised by the Nursing and Midwifery Council. The resulting hearing concluded that her role relating to Joshua’s death was serious enough to warrant a suspension from the professional register for 9 months. The hearing gave the trust a dilemma; should they continue to employ a member of staff who was unable to practice clinically and had been subject to heavy criticism relating to the preventable death of a baby, or should they dismiss her? Instead of rushing to make a decision that on face value, might have seemed like the right and ‘just’ thing to do, the trust asked if I might be willing to meeting the midwife to talk through what had happened and what had been learned. I agreed to do so.
In all the years that had passed since Joshua’s death, the only time I had been in the same room as any of the staff involved in his care was at Joshua’s Inquest (which occurred nearly 3 years later) and whilst giving evidence in formal Fitness to Practice processes. These were bureaucratic processes, determined by legal advice – cold, compassionless, and inhumane.
In preparation for the meeting I thought long and hard about what I wanted to say. I wanted to tell the midwife concerned that I didn’t blame her for the mistakes made in Joshua care and that I knew she didn’t intend for the outcome for Joshua to be what it was – but I also wanted to tell her how the lack of honestly afterwards had impacted on my life and of my anger that Joshua’s life seemed to matter so little.
When I walked into the room, after a few words of introduction by the facilitator – I was given the opportunity to talk directly to someone I thought of as caring very little about what happened to Joshua and the consequences on our family.
I only got through half of what I wanted to say… that I didn’t blame her for the mistakes that led to Joshua’s death…. but I could not get any further. The midwife broke down in tears and told me that every day since Joshua died, she had blamed herself for what happened – that she wished she had done things differently and that she would carry that for the rest of her life. It was not fake or rehearsed emotion and at that moment, the image I had in my mind of an uncaring and callous person disappeared. In an instant my anger lifted. We cried together and had a hug.
I left that meeting with a sense of healing but also profound sadness. Sadness that we weren’t able to meet much earlier and sadness that on the long journey since Joshua died – somehow humanity and compassion were sucked out of the process – at the very time when kindness was needed the most.
A recent and welcome movement in healthcare is the focus on ‘just culture’. If we genuinely want to make stories like Joshua’s a thing of the past, we must fundamentally change the way our healthcare system responds to error and harm.
If we get this right, the aftermath of patient harm will cease to be characterised by adversarial processes, denial and cover up that are so toxic to learning and improvement. Instead we can focus on the people who have been hurt and what they need to rebuild trust, to forgive and remember.
We will see a shift away from the hunt for individual blame allowing a much greater focus on the most important accountability of all – that which is owed to future patients to ensure they don’t come to harm through the same mistakes happening again.
James Titcombe – 17th September 2020